

Theme: In an ever more connected and interdependent world, the outbreak of an infectious disease in one country could actually become a health emergence of concern for the entire world. The following analysis assesses the potential risk of several emerging and re-emerging infectious diseases. The analysis gives as a conclusion a list of actions to be adopted in order to prevent, control and minimize such an increasing threat.
Summary: In this analysis, I address the different factors influencing the emergence of infectious diseases all around the world in the context of a globalised society. The economic and political consequences of globalization are strongly linked to the re-emergence of infectious diseases. High demographic growth (See Fig. 1), poor health education, human displacements due to local wars, uncontrolled exploitation of natural habitats and social instabilities are different faces of globalization that create the conditions for the emergence and the rapid transmission of infectious agents. After that, I compile quantitative information about the increase of infectious diseases both in developing and developed countries, and I try to assess the different indirect and direct potential threats of each disease, in particular, for Spain and Europe in their capacity of being important actors in our global society. Finally, I summarize the main threats and challenges we face and the measures that need to be undertaken in the following years to prevent new emerging diseases, such as SARS, re-emerging food-borne diseases, antimicrobial resistance, AIDS and tropical diseases, such as malaria, yellow fever and dengue, from spreading and prospering. I conclude by stressing the important role that Spain can play to increase control and prevention of infectious diseases; not only because Spain acts as an immigration gate to Europe, receiving a lot of people from Latin America and North Africa every year, but also because Spain is strategically located to play a leading political role to increase co-operation with developing countries in public health affairs, particularly in Latin America.
Figure 1 Evolution of human population*.
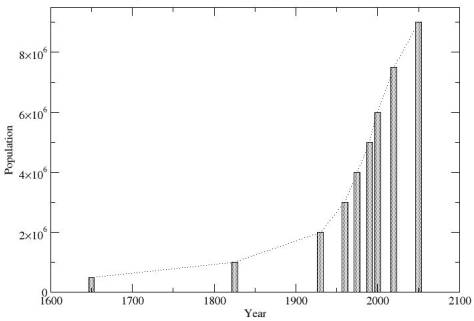
* Redrawn from Laurance, 2001, TREE, 16:531-533
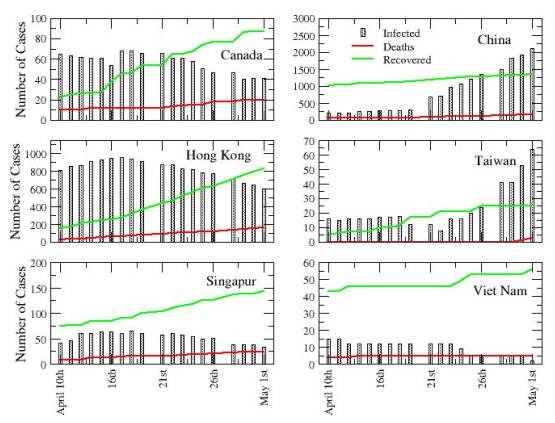
Analysis: When some people started dying from what initially looked as a usual flu in Guangdong (China) last November, nobody expected that some months later (May 2nd) there would be a cumulative total of 6,054 probable SARS cases, a total death toll of 417 from the disease, and that it would have spread to over 27 countries in Asia, Australia, America and Europe (See Fig. 2). However, the case of the severe acute respiratory symptom (SARS) in China is not an isolated event. The spread of the virus is just a new example of the consequences of our increasing globalised world, where the risk for the spread of new infectious diseases is rising rapidly.
Figure 2. Evolution of SARS in epidemic countries, i.e., those where local transmission took place. Data from WHO. May 2003.
For example, between February and November 2001 around 20% of the total number of outbreaks of infectious diseases communicated to the WHO were caused by unknown, probably new infectious agents. An example of such outbreaks is the number the outbreaks of Ebola haemorrhagic fever. The Ebola outbreaks are especially famous due to their high case-fatality rate. Ebola arose for the first time in the Democratic Republic of Congo (September 1979) and then in Uganda (October 2000). In both cases more than half of the affected population died from the infection. Very recently it has started to spread again in Congo (May 6th 2003, 143 cases, including 128 deaths). Other severe outbreaks threaten public health every year. Cholera, for example, is a well-understood and easily treatable disease. Despite this, it is still a persistent threat in developing countries, where infectious diseases transmitted by contaminated food and water is a constant and frequent threat to health often with fatal consequences. AIDS remains as a global pandemic in Africa and Asia, and vector-transmitted diseases (yellow fever, malaria and dengue) are re-emerging with increased intensity every year in tropical areas. As result of this, the public concern regarding the global threat of rapid spread of infectious diseases is growing. International organizations, such as the World Health Organization (WHO), are trying to respond to these growing concerns, and in May 2001 the WHO adopted a resolution on “Global health security: epidemic alert and response”, which particularly acknowledges the link between globalization and the recent upsurge of infectious diseases.
At the beginning of the twentieth century, infectious diseases were the leading cause of mortality worldwide. Since then, the technological and medical advances have reduced the incidence of infectious diseases to very low levels in the developed part of the world. Safer food and water, better housing, better nutrition, and better sanitary conditions, together with the extensive use of vaccines and antimicrobials, were the main factors influencing the constant decrease of infectious diseases during the last century. By the end of the century, the leading cause of death were no longer infectious diseases but chronic illnesses, such as heart disease and cancer, responsible for about half of the total number of deaths. By contrast, the developing world did not see the same positive development regarding the impact of infectious diseases. In 1998, the WHO estimated that infectious diseases caused over 13 millions deaths in the developing countries –approximately a quarter of the total number of deaths in 1998 worldwide-. Among the most common causes of death were the same three diseases that had been responsible for much of the excess mortality in the developed part of the world at the beginning of the twentieth century: pneumonia, diarrhoeal disease and tuberculosis, which sadly enough is affecting mainly small children. Thus, the great scientific and technological progress during the last century did not reach the developing world. In spite of international efforts to improve this situation, such societal and medical advances have had little effect.
The main causes of this unfortunate and unbalanced development stem from the economic differences arising from the global economic system, which is based on the assumption of maximizing profits. A simplified but nevertheless essentially true picture can be described as follows: Developed countries sell expensive technology to developing countries. The economically weaker developing countries, in turn, provide resources and raw materials at cheap prices to developed countries. Thus sustaining their further economic growth. Part of the benefits from this unbalanced trade is returned to the poor countries in the form of loans. To repay these, poor countries face selling their resources at continued low prices or borrowing more money. The result of this debt trap is an increasing “development gap” between rich and poor countries that impede many poor countries from setting aside the necessary resources, in particular, for combating infectious diseases, for which cures are available, and improve their general health conditions to prevent future outbreaks. It is also responsible for the political and social instabilities that, in scenarios of deficient public health systems, are very often primordial causes for the rapid spread of infectious diseases. In other words, if the poor countries only had the means for combating infectious diseases, several million lives would be spared each year.
Figure 3 Increase in resistance to antimicrobial agents. Percentage of reported cases of gonorrhoea caused by antibiotic resistant strains *.
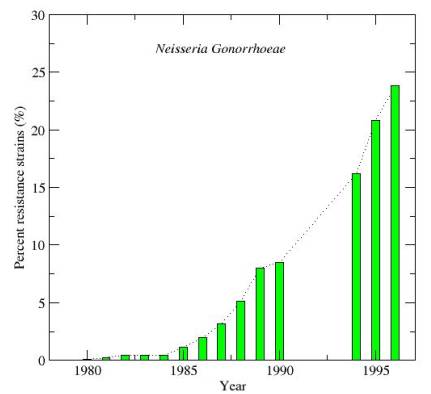
* Redrawn from Brock et al (1994), “The biology of micro organisms” with more recent data from URL: http://www.cdc.gov/ncidod/dastlr/gcdir/gono.html.
There are good reasons that explain why the developed world should be sensitive about the situation in the developing world. The effects of the failure to combat infectious diseases globally instead of only regionally, i.e., in the developed part of the world, is starting to have fatal consequences for the global health situation. In recent years, infectious diseases are re-emerging both in the developing and developed world, and mortality rates due to infectious diseases are on the rise again in the developed world after having declined for more than a century. During the last part of the twentieth century, new infectious agents have been identified. The HIV and Ebola viruses are just striking examples. Diseases such as cholera, tuberculosis, dengue fever, yellow fever and malaria, which had once been controlled in many parts of the world, are also re-emerging. Resistance to antimicrobial agents is becoming a serious global problem (See Fig. 3). Once easily treatable infections are starting to become a serious threat for health in all parts of the world, what are the factors influencing the emergence of infectious diseases? Three broad groups of direct causes can be identified:
1.Increased risk for transmission of diseases. Our developed world is facilitating long-distance transmission as a result of international travel and trade. The case of Toronto (Canada), the only city in a Western country where the SARS epidemic has spread locally, is a clear example. Although the increase in contacts across cultures and continents is producing an increased risk in transmission of diseases at a global scale, in developing countries local disease transmission is relatively more important and is mainly linked to the breakdown of public health measures, the lack of sanitary conditions and mass human migrations as a consequence of natural or man-made catastrophes.
2.Increase in people’s susceptibility to contract a disease. The number of people susceptible to infections is increasing rapidly in the developed world as a consequence of the aging process (see also another Analysis of the Royal Institute “The Ageing of the Population (part I): Scope and Future Outlook in Spain” by Rickard Sandell). With an aging population, there are more persons that are susceptible to certain diseases and larger groups that can sustain transmission. Under these conditions, once started, the spread of new infections become more difficult to control. By contrast, in the developing world increasing susceptibility is mainly due to interaction between diseases. For instance, the increase of tuberculosis is clearly linked to AIDS in Africa. People suffering from AIDS are prone to acquire other infections, and, in so doing, they can easily sustain disease transmission.
3.Environmental and ecological change. Infectious diseases will remain an ever-changing problem for human public heath. Infectious diseases are the result of a host-pathogen interaction subjected to co-evolution. Host defences tend to increase against virulent pathogens in a sort of arms-race. For instance, human populations living in areas where malaria has been endemic for centuries are more resistant to the illness. Environmental changes are responsible for shifts in the geographical distributions of organisms in general and parasites in particular. When these shifts occur, the carrier of the infectious material may attack populations that are less resistant than populations traditionally exposed to the infection. Furthermore, changes in technology and industry have also made a strong influence on the environment. Take the production of food, for example. Using antimicrobial agents for promoting animal growth and preventing diseases has facilitated low-cost food production, but at the same time it has contributed to the emergence of drug resistance to antimicrobials that may eventually reach humans through the food chain. An exaggerated use of antimicrobial in developed countries has also contributed to the selection procedure giving rise to increased resistance against antibiotics of bacterial infectious agents.
What are the diseases we should be most worried about? Below, I list the main epidemic-prone diseases that challenge global public health nowadays. They belong principally to two different categories. The first category includes those diseases that have a high probability to become dangerous also in our latitudes, such as for example, new emergent diseases, influenza, epidemic meningitis and some sporadic food-borne diseases. The second category includes diseases that have shown a spectacular increase in recent years in developing countries. Hence, it is worth assessing their potential threats in order to design control and prevention strategies oriented both to our public health system and to help the strongest affected countries. It is worth noticing, however, that developing countries are equally threatened by any of the following diseases in the two categories.
1.New emergent diseases. The recent event of SARS has shown that there is no country completely safe against the invasion of a new emergent infectious agent. The agent causing SARS belongs to the Corona virus family, which is widespread in animals, but frequently found also in humans. Human Corona viruses are one of the main causes of the common cold. The origin of SARS virus is not known yet. With a case-fatality rate of around 5%, no treatment is available to fight the infection. In such situations, controlling further transmission of the illness is the only measure to stop the spread of the infection. Surveillance, preparedness and rapid action are the only tools available in order to fight effectively against such episodic events.
2.Influenza. A virus causes this common infection, which is able to elude our immunological defences by presenting new mutations every year. Usually, the virus genetic content undergoes what is called antigenic drift. This means that the virus genetic content is very unstable and undergoes constant mutations. This is an efficient mechanism to prevent humans and animals from developing an effective resistance to the virus. Our immunological system offers some protection, and it can retain immunity depending on how similar mutant viruses are to viruses from past years. However, rarely, and in a very unpredictable way, the virus undergoes what is called an antigenic shift. This process involves a swapping of genetic material from different virus particles resulting in a novel virus subtype. Viruses transformed in this way are completely different from both parent viruses. As a consequence, populations will have no immunity to the new virus subtype. In the last century, three huge influenza outbreaks correlate with three antigenic shifts. The first outbreak occurred in 1918 and caused 40 million deaths all around the world. The second and the third outbreak, in 1957 and 1968, caused around 4.5 million deaths. Experts say that nobody can predict when the next antigenic shift will occur. What is clear is that the potential danger of such an event is out there. Given our globalised society, the spread of a “new” influenza virus could have unprecedented consequences not only in terms of deaths, but also as a huge disruptive cause with serious impact on travel, tourism and trade.
3.The AIDS epidemic that appears to be under control in the industrialized world is still out of control in developing countries. Only in 2001, 3.5 million people were infected in sub-Saharan Africa, where a total number of 28,3 million people currently live with AIDS/HIV. Such figures urgently demand firm actions from our industrialized economies. (The consequences of the AIDS pandemic will be addressed in a further analysis).
4.Bacterial meningitis causes inflammation of the membranes enveloping the brain and spinal cord. Different bacterial agents can cause such an inflammation. In principle, it is treatable, but the rise of drug resistance of many bacterial strains has greatly compromised the success of medical cure. The case-fatality rate is 5-10%, but, among survivors, between as much as 10-20% suffer permanent brain damage. The most important meningitis germ causing sporadic cases and small outbreaks throughout the world is Neisseria meningitidis. Bacteria are readily transmitted through coughing or sneezing or through close facial contact. Recurrent epidemics show cycles at intervals of 8-12 years. Since the early 1980’s, amazingly, the intervals between epidemics have become shorter and highly unpredictable. Neither the causes of those historical cycles nor the changing patterns are currently fully understood. What is clear is that travel and migration facilitates the circulation of virulent strains within and between countries, and large population movements linked to religious pilgrimages have been documented to be causes of both regional and global spread.
5.Food-borne diseases are transmitted by contaminated food and water. In the developing world the best strategy to fight against them is to improve food and water safety by preventing faecal contamination of human food. Diarrhoeal diseases are estimated to cause 1.9 million deaths mostly in children. In developed countries, food-borne diseases are also a threat. Although, when occurring they are usually mild infections without fatal consequences. However, emerging new pathogens and widespread drug resistance could complicate this situation. We should keep in mind that, due to an increasing technification in food production, we are more and more dependent on others to ensure the safety of our food.
6.Cholera is an acute intestinal bacterial infection characterized by profuse watery diarrhoea, vomiting and rapid dehydration. Cholera is easily treated by prompt oral or intravenous administration of salt fluids, but if left untreated, it can kill within hours following the onset of symptoms. The last huge cholera outbreak in the last 15 years occurred in 1991. It affected Asia, Africa and America. In America 400000 deaths were reported in 11 countries in just one year. Cholera is strongly linked to poor sanitation, crowded living conditions and contaminated water resources. Those conditions are frequently met in many developing countries but less often in the developed world. Thus, Cholera remains an endemic problem in many areas of the world, where the number of explosive outbreaks linked to natural disasters, wars and crowded refugee camps is actually increasing.
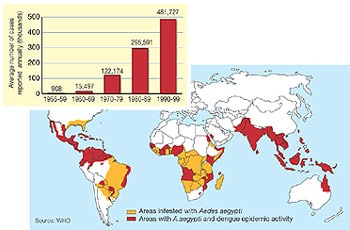
7.Yellow fever, dengue and malaria. A mosquito transmits these three tropical illnesses. Mosquitoes are first infected by the micro parasite, which thereafter pass it on to humans while feeding on human blood. Yellow fever is by far the most efficient killer, with a case fatality rate approaching 85%. Dengue is a re-emerging epidemic prone disease transmitted by the same mosquito species as yellow fever, but less mortal (1-5% case-fatality rate). Frequent outbreaks of both diseases are increasing in number recently (see Fig. 4). By contrast, malaria is well spread, almost endemic, particularly in Africa, where there are up to half a billion cases every year and about 2 million deaths –half of those are children in sub-Saharan Africa-. No treatment exists for dengue or malaria. The vaccine for yellow fever is highly effective and confers immunity at least for ten years. Unfortunately developing countries cannot afford an extensive immunization campaign for a disease that remains largely invisible between highly unpredictable outbreaks.
Figure 4 Increase in dengue all around the world from Nature (18 April 2002) “news feature”
Conclusion: Given the general disease outlook described above, in an ever interconnected and interdependent globalised society: What are the priorities to be made in order to address emerging infectious diseases in the twenty-first century?
Even though the most suitable strategy may vary from problem to problem and from country to country, some common guidelines are shared and strongly recommended by all international health organizations:
1.Enhancing surveillance and rapid response. It is worth noticing that unpredictability is a common trait of emerging infectious diseases. Thus, the degree of preparedness is crucial to stop infection transmission.
2.Encouraging and funding scientific research. Intensive research on new antimicrobial agents, vaccines and immunology is needed. Genetic, ecological and evolutionary studies oriented to improve our understanding of host-germ interactions should also be funded.
3.Funding public health systems, strengthening the interconnection of health and research centres, and providing training opportunities. To some extent an epidemic outbreak can be compared to a fire in a forest, with the only difference that the trees would be highly mobile. However, while there are well-prepared firemen ready to act just in case of a fire in a forest, there is no well-trained and flexible work-force ready to intervene when infectious diseases emerge.
4.Developing, implementing and evaluating strategies for prevention and control, including public health education programs to increase the general awareness of, and how to deal with, the potential danger of infectious diseases
Although the above-mentioned guidelines are urgently needed, they are just actions designed to dampen the effects of the true problem. None of the points mentioned is oriented to improve the economical situation of developing countries. The true problem underlying the re-emergence of infectious diseases all around the world lies on our current global model of economic development, which is environmentally impossible to sustain for many years, and which is creating an ever deeper gap between developed and developing countries, resulting in a constant source of social and political instability. Spain, due to its historical link with Latin America, could play a leading role in Europe to reinforce political cooperation with developing countries in public health affairs, education and scientific research in order to counterbalance the increasing globalizing trend characterized by economically centered international relationships.
David Alonso
physicist and biologist. At present, he is working on stochastic modelling of ecological systems with strong interest in the ecology of host-pathogen interactions.